
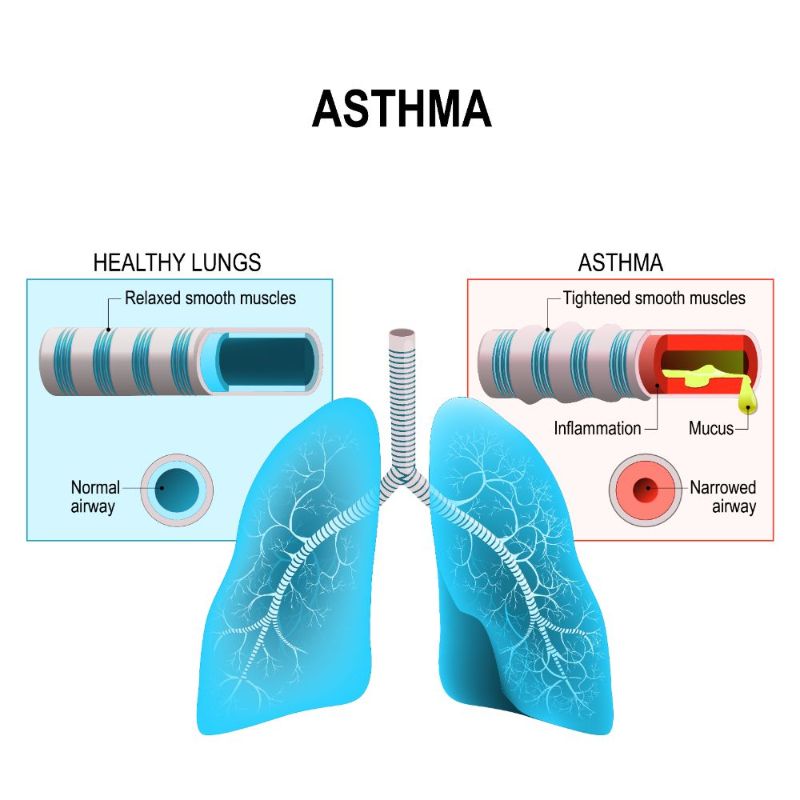
Asthma is an inflammatory airway disease characterized by wheezing, shortness of breath, cough and chest tightness. It affects about 300 million people globally from all age groups, with an increasing prevalence in developing countries. Viral infections, allergens at work or home like house dust mite, pollens etc., smoking, exercise and stress are the main factors that trigger or worsen asthma. The main aim of treatment of asthma is to achieve ‘control᾿ of symptoms. This includes minimal daytime and nocturnal symptoms with ability to perform any physical activity without much limitation.
Inhaler therapy with corticosteroids is “the treatment” to attain asthma control. However it is often noted that, patients visiting us are frightened by the very word “asthma” and they will be asked an array of questions like “will my asthma be cured ?”, “ will I be addicted to inhalers?” etc . These questions are myths that need to be busted. World Asthma Day celebrated on May 5 2021 is based on the theme “ Uncovering Asthma Misconceptions”. Hence this article comes with an aim to focus on some common myths on asthma and their real facts .
“Inhaled corticosteroids are the mainstay of treatment.”
MYTH #1: Asthma can be cured.
FACT: Asthma can be well controlled.
Asthma is a chronic condition with the symptoms varying over time and can be intermittent or disappear due to changes in the body or environment. The treatment of asthma is aimed at optimum control of symptoms. Inhaled corticosteroids are the mainstay of treatment. If the asthma is well controlled on assessment by a regular follow up every 1-3 months , inhaler therapy can be stepped down from a ‘daily regimen ᾿ to even ‘as and when needed regime᾿. However, symptoms can resurface at any time and stepping up off treatment may not be completely eradicated.
MYTH#2: Asthma medications need to be taken only during symptoms.
FACT: Asthma medications need to be taken regularly with tailoring of treatment based on patient’s ‘asthma control᾿ when regularly followed up by a pulmonologist.
Asthma medications i.e. inhalers are divided into two – controller and reliever. Controller inhalers containing inhaled corticosteroids which need to be taken regularly and are necessary for asthma control. Reliever inhalers can be used during flare up of symptoms as and when required. The current ‘SMART’ therapy (Single Maintenance And Reliever Therapy) mentions the use of corticosteroid-containing inhalers as both controller and reliever therapy. These controller inhalers need to be taken regularly to achieve a well controlled asthma.
“To date, evidence for the use of Artificial Intelligence (AI)-driven decision support in clinical settings for chronic disease management remains limited. Data visualisation, or linked decision-support advice/ alerts can empower end users, i.e. turn data into knowledge and action. Clinical decision support (CDS) provides timely information, usually at the point of care, to help inform decisions about a patient’s care.”
MYTH #3: Physical activity/ sports should be limited if you have asthma.
FACT: A well controlled asthma allows you to lead a normal, healthy life – including regular exercise .
As mentioned earlier, a well controlled asthma enables us to perform any physical activity with ease. If you have any difficulty in performing a physical activity it means that your asthma is not in control. In fact regular exercise prevents obesity, makes your heart and lungs stronger and improves your immune system. Obesity makes asthma control difficult. It is noteworthy to mention sportsmen like David Beckham and Michael Phelps who overcame asthma, thus emphasising a combination of exercise and medication for good control.
MYTH #4: Inhalers can be addictive.
FACT: Inhaled corticosteroids are not habit forming / addictive.
Corticosteroids used in inhalers are a copy of the steroids that are normally produced in our body. Regular use of these medications does not cause addiction and are often needed to bring down airway inflammation and achieve asthma control. Early discontinuation can cause symptoms to reappear and hence should be used as prescribed by the doctor.
“Corticosteroids in inhalers are in microgram doses as compared to tablets/ syrup which are in grams. “
MYTH # 5: Inhalers are ‘strong medications’ and are the last resort for the treatment of asthma.
FACT: Inhaled corticosteroids are the first and the best medication to control symptoms with steroid doses in micrograms.
Inhaled corticosteroids are the cornerstone in the treatment of asthma. Corticosteroids in inhalers are in microgram doses as compared to tablets/ syrup which are in grams. Moreover as they are inhaled, they provide rapid relief of symptoms and reduction in airway inflammation needed to achieve control.
“a very minuscule percentage of children with asthma on regular inhaled steroids have 1 to 1.2 cm less height than their normal percentile in the long term.”
MYTH #6: Inhaled steroids cause weight gain, increased blood sugars, growth stunting in children and other side effects as seen in oral steroids.
FACT: Inhaled steroids reach our lungs only in minimal amounts with no systemic side effects.
As mentioned previously, inhaled corticosteroids are available in microgram doses. On inhalation only ῀ 20% of this dose will reach our airways and lungs with the systemic absorption being almost nil. Hence systemic side effects as seen in oral steroids are never present.
With regard to stunting of growth in children, studies have shown that a very minuscule percentage of children with asthma on regular inhaled steroids have 1 to 1.2 cm less height than their normal percentile in the long term. BUT, it should be remembered that if asthma is uncontrolled then the reduction in height can be much more.
These are the common myths faced by us which have to be communicated appropriately. Therefore an early diagnosis of asthma and an adequate treatment plan with inhaled steroids can help any individual lead an active, normal and unrestricted life without impeding physical and psychological development .
“Dr. Mitchelle Lolly is a pulmonary specialist and is currently in Kochi.”